A 16Y old with uncontrolled sugars
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
She was apparently alright 10 years back , one day she suddenly had fever with chills and burning sensation all over the body for which got diagnosed as DM-type 1 on routine investigations
She is on regular medication since then on INSULIN(ISOPHANE-10u+REGULAR INSULIN 10u)
After 6yrs of regular medication she missed her doses on and off for which she got admitted in the hospital with c/o vomitings ,SOB and burning micturition .necessary treatment was given and discharged
2 years back ,Hospitalised for 1 week with similar complaints of vomitings, SOB . She got discharged with dietary counselling and insulin dosage advice
1 year back , she got admitted with c/o fever, SOB (grade4)and acidotic breathing .ABG showed severe metabolic acidosis and ketones were positive. She was intubated and connected to mechanical ventilation . She was started on iv fluids and iv insulin algorithm 2 for management of DKA , extubated after 3 days .
Now,She had c/o vomitings and pain abdomen since 4 days
Pain in epigastric region , dull aching type, non radiating,no aggrevating and relieving factors
Vomitings since 4 days ,3-4 episodes, non projectile, non bilious,contents being food particles
She had fever ,high grade,intermittent type associated with chills and rigors
Noh/o burning micturiton, sore throat,cough, confusion, loose stools, constipation,polyuria, polydipsia
HABITS: mixed diet, normal appetite, adequate sleep,no addictions,bowel and bladder movements are regular
FAMILY HISTORY: no similar complaints
Her grand father is a k/c/o DM
GENERAL EXAMINATION: pt is c/c/c moderately built and nourished
No pallor, icterus, cyanosis, clubbing, koilonychia, pedal edema
VITALS: temp- afebrile
BP- 110/60mmhg
PR- 104bpm
RR- 25cpm
Spo2-99%on room air
SYSTEMIC EXAMINATION:
P/A: shape of abdomen- scaphoid, umbilicus- inverted
Soft, tenderness present, bowel sounds heard
CVS: s1 s2 heard, no murmurs
RS: BAE clear,no added sounds
CNS: higher mental functions are intact
Cranial nerves: intact
Motor system: intact
Sensory system: intact
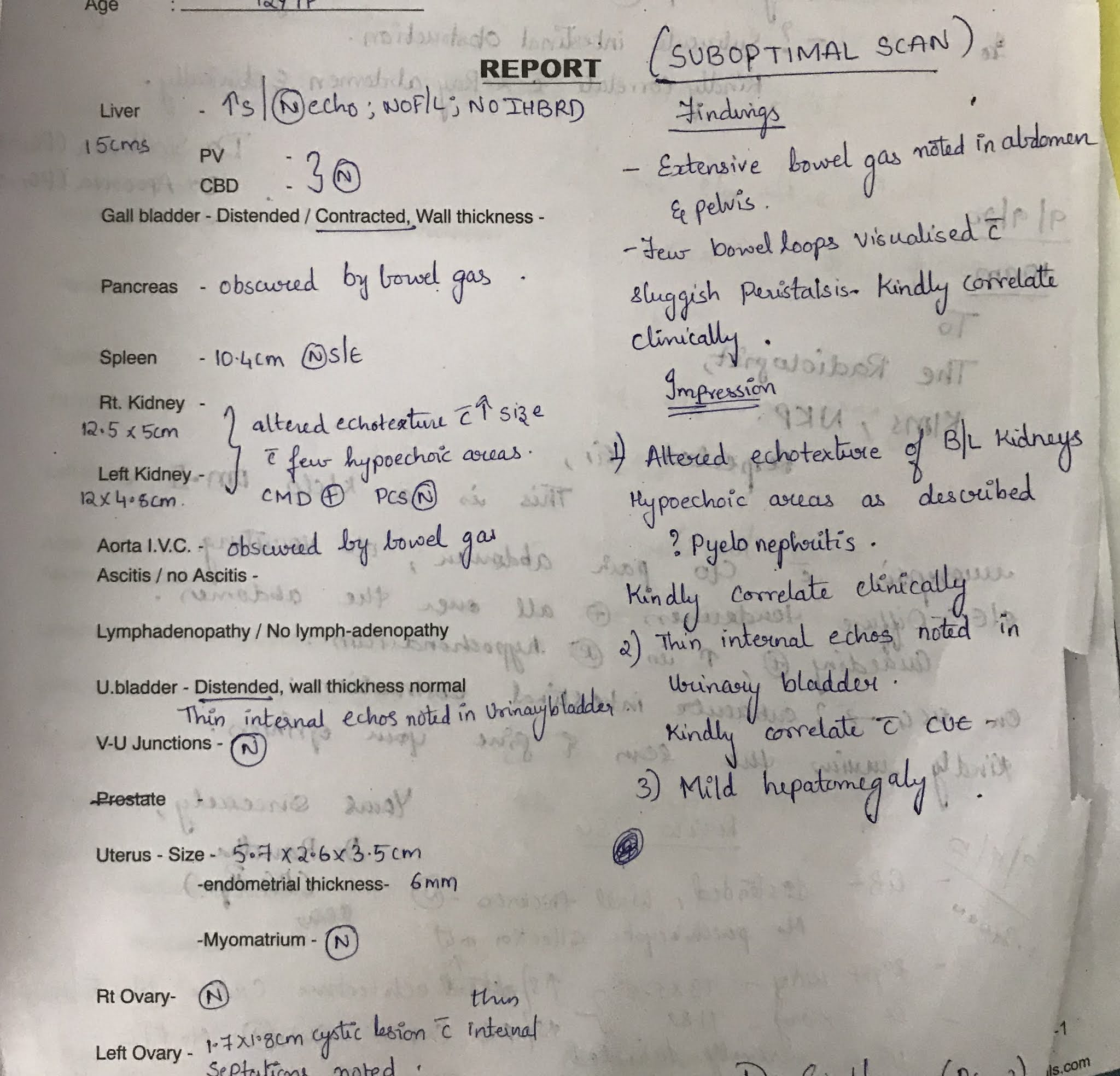
INVESTIGATIONS:
RBS:288mg/dl
FBS:227mg/dl
Hba1c:6.8
LDH:277
Serum amylase:24
LFT:
Total bilirubin:1.42
Direct bilirubin:0.17
SGOT:12;SGPT:10;ALP:305
Total protein:5.6;albumin:2.3;A/G:0.68
RFT:
urea:21 creatinine:0.7 uric acid: 3.6
Ca :9.7;phosphorus:3.9 na+:133 k+:3.4 cl-:95










Comments
Post a Comment